Public Information on Fecal Incontinence
What Is Continence, and How Does the Bowel Work?
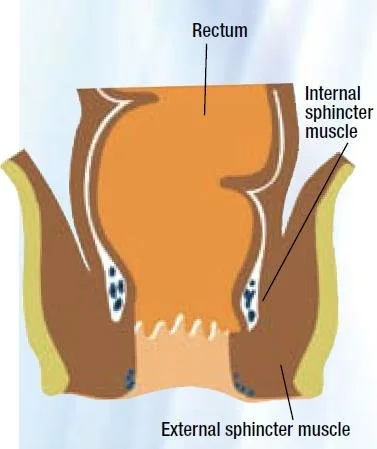
Continence means having control over when and where you pass urine or stool. Bowel control depends on several parts of the body working together. As food is digested, waste moves through the intestines and is stored in the rectum. When the rectum fills, nerves send signals to the brain, creating the urge to have a bowel movement. The muscles around the anus and pelvic floor tighten to hold stool until it is socially appropriate to use the toilet. When you are ready, these muscles relax, allowing the bowel to empty.
What Is Fecal (Anal) Incontinence?
Fecal incontinence (also called anal incontinence) is the involuntary loss of stool (and/or gas). It may occur:
Occasionally or regularly
With little or no warning
During daily activities or during sleep
Some people may experience:
Difficulty holding gas
Small amounts of stool leakage
Strong urgency and not reaching the toilet in time
Types of Fecal Incontinence
Anal incontinence is commonly described in three types:
Passive Incontinence: Stool or gas leaks without the person being aware it is happening. This is often due to reduced rectal sensation or weakness of the anal muscles.
Urge Incontinence: There is a sudden, strong need to have a bowel movement, but the person cannot reach the toilet in time. This is often related to muscle weakness, poor coordination, or loose stool.
Soiling (Post-Defecation Leakage): Small amounts of stool leak after a bowel movement, often due to incomplete emptying of the rectum or difficulty with anal closure.
Common Causes of Fecal Incontinence
Weakness or damage to the anal and pelvic floor muscles (e.g., childbirth, surgery, aging, long-term straining)
Nerve damage or reduced nerve function affecting bowel sensation or control
Loose stool or chronic diarrhea
Constipation with overflow
Reduced rectal sensation
Reduced ability of the rectum to store stool
Bowel conditions such as irritable bowel syndrome or inflammatory bowel disease
Side effects of certain medications, including some laxatives or antibiotics
Who Can Help with Fecal Incontinence?
Primary Care Provider (Family Physician or Nurse Practitioner )—assessment, advice, and referrals
Pelvic health physiotherapist – pelvic floor muscle training, bowel control strategies, and education
Gastroenterologist – medical specialist in assessment and treatment of bowel condition
Colorectal surgeon (also called proctologist)- treat diseases of the colon, rectum, and anus.
General surgeon -performs a wide range of surgical procedures in the abdomen and digestive tract
Continence nurse or nurse specialist—education, skin care advice, and continence support
Community health or primary care teams—coordinated care and access to local services
When Should You See a Healthcare Provider?
Bowel leakage occurs more than occasionally
Strong urgency prevents reaching the toilet in time
Symptoms interfere with work, social life, or daily activities
You avoid leaving home due to bowel control concerns
Symptoms are worsening or not improving
Skin irritation or discomfort is present
You feel worried, distressed, or unsure how to manage symptoms
How Can Fecal Incontinence Be Prevented and Managed?
Try to use the toilet at regular times, and don’t rush or strain. Go when you feel the urge.
Eat a healthy diet with enough fiber and increase it slowly so your body can adjust.
Drink plenty of water every day to help your digestion.
Avoid foods that make your symptoms worse.
Take care of constipation or diarrhea early—talk to a healthcare professional if needed.
Do pelvic floor exercises to strengthen the muscles that help control your bowels. A pelvic health physiotherapist can show you the best exercises.
Sit on the toilet with your feet on a small stool, lean slightly forward, and try to relax while breathing normally.
Stay active with regular physical activity.
See a doctor if you notice any changes in your bowel control.
Fecal Incontinence: Myths and Facts
Myth: Only older people have fecal incontinence
Fact: It can occur at any age and may follow childbirth, surgery, nerve injury, digestive problems, or pelvic floor weakness.
Myth: It doesn’t happen very often
Fact: It is more common than people think, but many do not talk about it due to embarrassment.
Myth: There’s nothing that can be done
Fact: Many people improve with treatments such as pelvic floor physiotherapy, bowel training, diet advice, and lifestyle changes.
Myth: Surgery is the only treatment
Fact: Most people do not need surgery. Conservative treatments are usually tried first.
Myth: Fecal incontinence means poor hygiene
Fact: This is a medical condition, not a personal failure.
Myth: Mild symptoms don’t need treatment
Fact: Early treatment can prevent symptoms from worsening and improve quality of life.
Myth: Pelvic floor therapy is only for bladder problems
Fact: Pelvic floor physiotherapy also helps with bowel control.
Myth: It’s too embarrassing to talk about
Fact: Healthcare providers discuss this every day. Talking about it is the first step toward improvement.
Additional Resources:
For more information on treatment options and a patient decision aid, see the World Federation on Incontinence and Pelvic Floor Disorders “Support in Continence platform” and decision aid guide for Fecal Incontinence options
References:
Bharucha AE, Dunivan G, Goode PS, Lukacz ES, Markland AD, Matthews CA, et al. Epidemiology, pathophysiology, and classification of fecal incontinence. Gastroenterology. 2015; 149(1): 53–64.
Rao SSC, Bharucha AE, Chiarioni G, Felt-Bersma R, Knowles C, Malcolm A, et al. Anorectal disorders. Gastroenterology. 2016; 150(6): 1430–42.
Dumoulin C, Cacciari LP, Hay-Smith EJC. Pelvic floor muscle training versus no treatment for urinary or fecal incontinence in women. Cochrane Database Syst Rev. 2018;10:
National Institute for Health and Care Excellence (NICE). Fecal incontinence in adults: management. Clinical guideline CG49. London: NICE; 2014.
Assmann, S. L., Keszthelyi, D., Kleijnen, J., Anastasiou, F., Bradshaw, E., Brannigan, A. E., Carrington, E. V., Chiarioni, G., Ebben, L. D. A., Gladman, M. A., Maeda, Y., Melenhorst, J., Milito, G., Muris, J. W. M., Orhalmi, J., Pohl, D., Tillotson, Y., Rydningen, M., Svagzdys, S., Vaizey, C. J., … Breukink, S. O. (2022). Guideline for the diagnosis and treatment of fecal incontinence—a UEG/ESCP/ESNM/ESPCG collaboration. United European Gastroenterology Journal, 10(3), 251–286.